

How Much Does In Home Supportive Services Pay
Summary. This post describes the Governor'due south budget assumptions and proposals related to the In‑Home Supportive Services (IHSS) program and offers relevant problems for Legislative consideration.
Background
Overview of the IHSS Plan. The IHSS program provides personal intendance and domestic services to low‑income individuals to assistance them remain safely in their own homes and communities. In guild to qualify for IHSS, a recipient must be anile, bullheaded, or disabled and in nigh cases take income below the level necessary to authorize for the Supplemental Security Income/State Supplementary Payment greenbacks assistance program (for instance, most $one,040 a calendar month for an aged and/or disabled individual living independently in 2021‑22). IHSS recipients generally are eligible to receive up to 283 hours per calendar month of aid with tasks such as bathing, dressing, housework, and repast training. Social workers employed past canton welfare departments behave an in‑home assessment of an private's needs in social club to determine the amount and blazon of service hours to be provided. In most cases, the recipient is responsible for hiring and supervising a paid IHSS provider—frequently a family fellow member or relative. The boilerplate number of service hours that will be provided to an estimated 598,000 IHSS recipients is projected to be 120 hours per month in 2022‑23.
IHSS Costs Split Between Federal Authorities, State, and Canton. IHSS costs are shared by the federal government, state, and county. Since IHSS primarily is delivered as a Medi‑Cal benefit, the federal share of cost is determined by the Medicaid reimbursement rate, which typically is 50percent. The state receives an enhanced federal reimbursement charge per unit for many IHSS recipients who receive services as a result of the Patient Protection and Affordable Care Human action expansion (90percent federal reimbursement charge per unit) and the Customs First Choice Choice waiver (56per centum federal reimbursement charge per unit). Overall, the constructive federal reimbursement rate for IHSS is about 54 percentage. The remaining nonfederal share of IHSS costs is covered by the state and counties. Historically, counties paid 35 percentage of the nonfederal share of IHSS service costs and xxx percent of the nonfederal share of IHSS administrative costs. Offset in 2012‑thirteen, however, the historical county share‑of‑cost model was replaced with an IHSS county maintenance‑of‑attempt (MOE), meaning county costs would reflect a set corporeality of nonfederal IHSS costs as opposed to a sure pct of nonfederal IHSS costs. The land is responsible for covering the remaining nonfederal share of costs non covered by the IHSS county MOE.
Budget Overview and LAO Assessment
The Governor'south budget proposes a total of $eighteen.5 billion (all funds) for IHSS in 2022‑23, which is almost $1.6 billion (9 percent) above estimated expenditures in 2021‑22. The upkeep includes well-nigh $six.5 billion from the General Fund for support of the IHSS programme in 2022‑23. Nosotros gauge that this is a net increase of near $2.8 billion (75 percent) higher up estimated General Fund costs in 2021‑22. This yr‑to‑year increase in General Fund reflects a much faster rate of cost growth relative to prior budget estimates. The chief reason for the year‑to‑yr Full general Fund cost increase is the anticipated ramp downwards of temporary increases to federal Medicaid funds (largely associated with the public health emergency) that were used to kickoff General Fund costs in the IHSS programme in 2021‑22. This ramp down results in roughly $ii billion in IHSS costs shifting back to the General Fund in 2022‑23. Additionally, the Governor's budget assumes continued twelvemonth‑to‑year growth in the 3 primary IHSS cost drivers: caseload (ii.8 per centum), hours per case (i percent), and IHSS provider hourly wages and benefits (3 percent). We describe in more detail central cost increases and toll shifts in this section.
IHSS Paid Caseload, Hours Per Case, and Hourly Wage Assumptions
LAO Bottom Line: Growth in IHSS Caseload Continues to Be Slower Than Pre‑COVID‑19 Rates. Caseload growth, a rise number of paid hours per case, and hourly wage increases for IHSS providers are fundamental drivers of increasing IHSS costs. Based on our analysis, we constitute that hourly wages and hours per case generally proceed to grow at a rate like to historical levels. However, we found that IHSS paid caseload continues to grow at a slower rate relative to pre‑COVID‑nineteen growth trends. Below, nosotros summarize our assessment of the paid caseload, hours per case, and hourly wage assumptions included in the Governor's budget.
Changes in Caseload Trends Before and Afterward the Onset of the Pandemic. Effigy 1 summarizes our assay of IHSS caseload trends before and after the onset of the pandemic. In general, the current average number of new applicants and denials are similar to pre‑COVID‑nineteen levels. In contrast, the average number of terminations are beneath pre‑COVID‑19 levels, which in function is due to the temporary pause of Medi‑Cal redeterminations (which we discuss in more detail in a subsequently section). Additionally, authorized cases continue to grow at a similar rate to pre‑COVID‑19 levels (iv per centum annually, or roughly 25,000 more than authorized cases every year). We constitute, however, that IHSS paid caseload is growing at a slower charge per unit since the start of COVID‑19 (from 4 percent annually to two percent in 2020‑21).
Figure 1
Cess of IHSS Caseload Trends
| IHSS Caseload Trend | IHSS Caseload Trends… | Comparing | |
| ...Before COVID‑nineteen | ...Since COVID‑19 | ||
| Average number of new IHSS applications | Around 17,000 in whatsoever given month. | Around 17,000 in any given calendar month. | Generally reflects pre‑COVID‑19 trends. |
| Average number of IHSS denials | Around 7,500 in any given calendar month. | Around vii,500 in whatsoever given month. | Mostly reflects pre‑COVID‑19 trends. |
| Average number of IHSS terminations | Around 9,000 in any given month. | Around 5,000 in any given calendar month. | Falls below pre‑COVID‑xix trends. |
| Average growth in authorized cases | Nearly 4 percent annually. | About four percentage in 2020‑21. | Generally reflects pre‑COVID‑nineteen trends. |
| Average growth in paid cases | About iv pct annually. | About 2 percentage in 2020‑21. | Falls below pre‑COVID‑19 trends. |
| IHSS = In‑Domicile Support Services. | |||
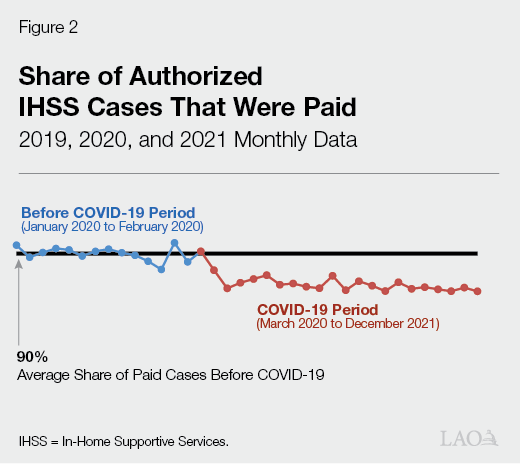
Continued IHSS Paid Caseload Growth, only at a Slower Rate. Prior to the kickoff of COVID‑19, the boilerplate number of IHSS paid cases has grown at an boilerplate rate of nearly 4 percent annually, reaching 555,000 in 2019‑twenty. The Governor'southward budget, nonetheless, assumes slower paid caseload growth in 2021‑22 (2.8 pct) and 2022‑23 (2.7 per centum). IHSS paid caseload began to grow at a slower rate in 2020‑21 (2.ane percent), which coincided with the showtime of the COVID‑19 pandemic (March 2020). Based on our analysis of caseload data, the slower growth in IHSS paid cases seems to be due, in part, to fewer authorized cases receiving paid services in whatever given calendar month since the start of COVID‑nineteen. Figure 2 shows that the average share of authorized cases that are paid every month slightly decreased from 90 pct to 88 percent since March 2020. This translates to roughly 14,000 fewer paid cases every month relative to pre‑COVID‑nineteen levels. Some of the reasons why authorized cases may not receive paid services include recipients not yet hiring an IHSS provider or existence temporarily hospitalized or admitted into a licensed care facility. Additionally, one possible COVID‑19‑related reason may be that recipients with non‑live‑in providers or not‑alive‑in providers themselves may be hesitant to collaborate with individuals outside of their household due to public health concerns. We are working with Department of Social Services (DSS) to go boosted IHSS caseload data and will provide farther comments at the time of the May Revision.
Continued Growth in IHSS Hours Per Instance. Since 2016‑17, the number of IHSS paid hours per case increased by about 2.5 per centum annually, reaching 118.7 hours per case in 2020‑21. The Governor's upkeep estimates that boilerplate hours per case volition remain roughly the aforementioned in 2021‑22 and slightly increase in 2022‑23 by 1 percent (to 119.6 hours per case). Based on recent growth trends, nosotros expect that the average paid hours per case volition continue to abound in 2021‑22 (as opposed to remaining roughly apartment). Additionally, we look the growth in average hours per instance in 2022‑23 to exist slightly higher than the administration'southward current estimate. We will go along to monitor the data related to IHSS paid hours per case and provide further comments at the fourth dimension of the May Revision if necessary.
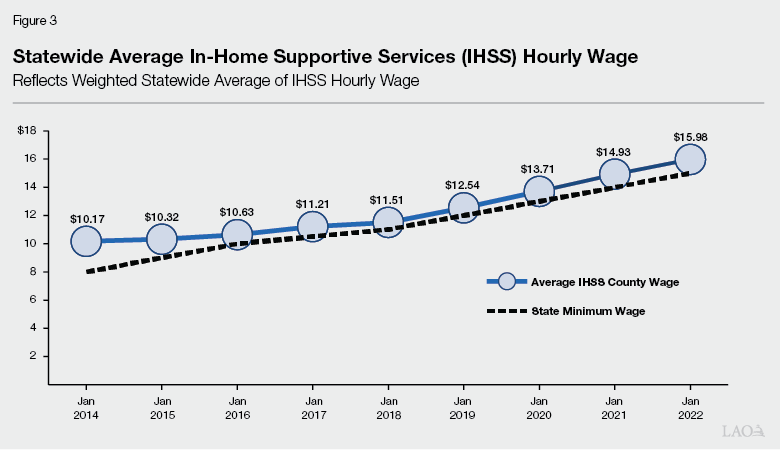
Connected Growth in IHSS Wages. As shown in Figure 3 , the boilerplate IHSS hourly wage has increased by 6 percent annually since 2014. The growth in IHSS hourly wages in part is due to increases to the country minimum wage—from $8 per hour in Jan 1, 2014 to $xv per hour in January one, 2022. Pursuant to current police force, the country minimum wage will remain at $15 per hour in Jan 1, 2023, increasing by inflation annually beginning January 1, 2024. Additionally, counties may establish IHSS hourly wages above the country minimum wage through local wage ordinances or, more than normally, collectively bargained agreements. As of January 2022, 50 counties accept IHSS hourly wages above the land minimum wage ($15 per hour). The Governor'southward budget includes well-nigh $400 million General Fund ($877 million full funds) in 2022‑23 for IHSS previously set, or agreed upon, wage increases. Specifically, this cost approximate partially reflects the full‑year impact of the state minimum wage increase to $15 per hour (effective January one, 2022). Additionally, the Governor's budget includes the full‑twelvemonth cost impact of locally negotiated wage increases above the $15 per hour state minimum wage.
Temporary Intermission of Medi‑Cal Redeterminations
LAO Bottom Line: Consider Means to Accost Unlike Treatment for IHSS Recipients Who Fail to Consummate Medi‑Cal Redetermination Once Federal Pause Expires. Medi‑Cal redeterminations were paused during the COVID‑19 public wellness emergency. Once Medi‑Cal redeterminations begin again, some IHSS recipients who do not complete their Medi‑Cal redetermination may motion to the IHSS‑Residual programme (fully state‑funded IHSS plan), while others may lose their eligibility for IHSS. The Legislature could consider ways to ensure all recipients receive the aforementioned treatment, which nosotros explicate in more than detail beneath.
Predictable Expiration of Temporary Pause of Medi‑Cal Redeterminations and Subsequent IHSS Terminations. Federal COVID‑xix‑related legislation effectively requires the state to append almost Medi‑Cal eligibility redeterminations for the duration of the national public health emergency declaration, which the Governor'south budget assumes will last until June xxx, 2022. While Medi‑Cal redeterminations are paused, essentially no IHSS recipient would demand to be eliminated from IHSS due to failure to complete their Medi‑Cal redetermination. This effectively reduced the number of terminated IHSS recipients and the number of IHSS recipients entering the IHSS‑Residual program. As a upshot, the Governor'due south budget assumes $xc one thousand thousand General Fund savings for the IHSS‑Residuum programme in 2021‑22.
Consider Possible Ways to Ensure Similar Treatment When Interruption on Medi‑Cal Redeterminations Expires. When IHSS recipients do not complete the Medi‑Cal redetermination procedure they tin can continue to receive their IHSS services through the IHSS‑Residue programme unless counties manually terminate them from the IHSS programme. Those that are terminated from the programme must reinstate their Medi‑Cal eligibility before receiving services again. Currently, there is no consistent arroyo to transmission terminations. As a issue, some recipients continue to receive services through the IHSS‑Rest program, while others practice not.
When the pause on Medi‑Cal redeterminations expires, in that location probable will be an increase in Medi‑Cal terminations due to beneficiaries not completing the redetermination process. We expect that in some cases, IHSS recipients terminated from Medi‑Cal will go along to receive services through the rest program, while others volition not. Equally a function of the 2021‑22 upkeep, the Legislature did not approve the administration's approach to accost this different treatment (which was to automatically finish all IHSS recipients who do not consummate their Medi‑Cal redetermination and require them to reinstate their Medi‑Cal eligibility before reentering the IHSS programme). Given the continued possibility of differing handling across similar recipients, the Legislature may want to consider the benefits and merchandise‑offs of alternative approaches to ensure similar treatment for all recipients. For example, the Legislature could consider ways to help IHSS recipients in completing their Medi‑Cal redetermination or provide temporary IHSS services for all IHSS recipients while they work towards reestablishing their Medi‑Cal eligibility.
Temporary Increase to Federal Medicaid Funding
LAO Bottom Line: IHSS Full general Fund Costs Expected to Increase in 2023‑24 equally a Issue of Expiration of Temporary Increment in Federal Medicaid Funding. Under the Families First Coronavirus Response Act, the federal regime increased the federal match rate for Medicaid services by 6.2 percentage points for the elapsing of the national public health emergency caused by COVID‑19. This increased federal lucifer lowers country costs for Medi‑Cal, IHSS, and other programs that rely on federal Medicaid funding. The Governor'due south upkeep assumes this enhanced federal funding is in identify from January ane, 2020 through June 30, 2022 and will offset $940 million in total IHSS Full general Fund spending in 2021‑22.
Additionally, under the American Rescue Plan (ARP) Act, the federal government increased the federal friction match charge per unit for IHSS and other Medicaid‑funded home‑ and community‑based services (HCBS) by an additional ten percentage points from April 1, 2021 through March 31, 2022. This increase in federal Medicaid funding is expected to beginning over $ane billion in baseline IHSS General Fund spending beyond 2020‑21 and 2021‑22. These savings will be transferred to the HCBS ARP Fund and spent on federally approved HCBS enhancements and expansions. The Governor's budget reflects the baseline IHSS savings and transfer of funds in the Department of Health Care Services upkeep.
Status of COVID‑19 Program Responses and Flexibilities
LAO Lesser Line: Consider Whether Sure COVID‑19 Program Flexibilities Merit an Extension. The state implemented numerous IHSS program flexibilities and enhancements to mitigate health and safety risks associated with COVID‑19. As shown in Effigy 4 , many of these plan flexibilities and enhancements have expired. Given that Omicron has go the prevailing COVID‑19 variant in California since the development of the Governor'south upkeep, the Legislature may desire to consider whether any IHSS programme flexibilities or temporary supports warrant an extension.
Effigy 4
Status of COVID‑19 IHSS Program Responses and Flexibilities
| Program Activity | Clarification of Flexibility | Cease Date |
| Active | ||
| Initial IHSS Cess | Counties may use video‑conferencing for initial assessment simply if an applicant or someone in the applicant's household has been infected with COVID‑19, has symptoms of COVID‑19, or has been exposed to COVID‑19 in the previous 2 weeks. In situations where at that place is less risk of COVID‑nineteen infection, counties should conduct initial assessment via an in‑person home visit. Counties may collect as much data every bit possible regarding the applicant over the telephone before the dwelling house visit to reduce the amount of fourth dimension spent in the applicant'southward home. | Terminate of the country of emergency in California |
| Almanac IHSS Reassessment | While counties are expected to begin to transition back to in‑person reassessments whenever possible, they may continue to utilize telephone and video‑conferencing to conduct almanac reassessments every bit needed. Additionally, earlier conducting an in‑person reassessment, counties may collect as much data equally possible regarding the applicant over the telephone to reduce the amount of time spent in the applicant's home. | End of the state of emergency in California |
| Submission of IHSS Programme Forms | When assessments and reassessments are conducted via telephone or video‑briefing, county staff may accept cocky‑attestations from applicants and recipients and/or their authorized representatives in lieu of original signatures on most required forms usually signed during assessments and reassessments. | Stop of the country of emergency in California |
| Submission of IHSS Provider Identification Documents | Temporarily waive requirement for IHSS providers to go to IHSS county or public authority office to present and photocopy original identification documents if function is closed. As an alternative, counties may have mailed‑in or faxed photocopies of the original identification documentation. | End of the country of emergency in California |
| Quality Assurance and Program Integrity | Counties may perform home visits for purposes of quality assurance and plan integrity remotely using telehealth, including video‑conferencing and phone. Specifically, counties should proceed to use video‑conferencing in situations where the applicant or someone in their household has been infected with COVID‑19, has symptoms of COVID‑19, or has been exposed to COVID‑nineteen in the two weeks prior to the home visit. In situations where there is no danger of COVID‑xix infection, the county can deport an in‑person habitation visit. | End of the state of emergency in California |
| Expired | ||
| Implement Agin Actions Related to IHSS Reassessments | Postpone the implementation of adverse deportment, such as reduction of IHSS hours and termination from IHSS program, resulting from the IHSS redetermination. | June 30, 2020 |
| Social Worker Outreach | IHSS and APS social workers perform out‑bound calls and/or visits to elderly recipients to ensure at‑take a chance recipients are receiving services they need and are condom in their homes. | June thirty, 2020 |
| IHSS Provider Criminal Groundwork Check | Temporarily suspend requirement for IHSS provider to complete fingerprint‑based criminal background check. As an alternative, counties may conduct name‑based criminal background checks. | July 31, 2020 |
| IHSS Paid Parent Provider Eligibility | Allow IHSS parent provider in ii‑parent household to go along to exist an eligible IHSS provider even if the second parent becomes a suitable care provider because the parent is not working or attending school or vocational program. | August 3, 2020 |
| In‑Person Provider Orientation | Temporarily suspend requirement for IHSS providers to complete in‑person provider orientation. | Baronial 31, 2020 |
| IHSS Provider Overtime Violations | Temporarily remove violations if IHSS provider worked above the commanded overtime limit. | August 31, 2020 |
| Federal COVID‑19 Paid Sick Leave | Provide boosted hours of paid sick exit for IHSS providers if they are unable to piece of work due to COVID‑19. | March 31, 2021 |
| Back‑Upward Provider System | Create a statewide emergency back‑up provider system with $2 per 60 minutes wage differential. | December 31, 2021 |
| COVID‑xix Vaccination Assistance | Pay IHSS provider to accompany IHSS recipient to their COVID‑19 vaccination date. | December 31, 2021 |
| Note: There is no set end appointment for the state of emergency in California. IHSS = In‑Home Supportive Services and APS = Adult Protective Services. | ||
Permanent Back‑Up Provider Organisation
LAO Lesser Line: Consider Possible Ways to Address Gap in IHSS Back‑Up Provider Services Given Delay in Permanent Back‑Upward Provider System. The emergency back‑up provider system expired on December 31, 2021. While the permanent dorsum‑upwardly provider system was intended to take upshot on January ane, 2022, because no program structure has been set in statute yet, the start date has been delayed to July ane, 2022. Equally a result, there is a current gap in back‑upwardly provider services. Below, we depict possible ways the Legislature could address this gap in back‑upward provider services.
Defective Statutory Structure, Permanent Back‑Upwards System Delayed. At the start of the COVID‑19 pandemic, the state created a temporary back‑upwards provider system to assist IHSS recipients when their regular provider could not piece of work due to circumstances related to COVID‑19. The temporary COVID‑19 back‑up provider system expired on Dec 31, 2021. The 2021‑22 budget included $5 million General Fund to create a permanent back‑up provider organization on January 1, 2022, contingent on a policy framework existence adopted in statute. However, a policy framework for the permanent back‑up provider system has non yet been adopted, resulting in a lapse in statewide back‑up provider services. (Some counties are standing to provide back‑up provider services despite the expiration of the temporary COVID‑19 back‑up provider system.) We understand that the administration intends to advise trailer bill linguistic communication—effective July one, 2022—outlining the program structure for the permanent dorsum‑up provider system. The Governor's upkeep includes $11 million General Fund in 2022‑23 to implement the permanent dorsum‑up provider system on July 1, 2022.
Possible Ways to Accost Gap in IHSS Dorsum‑Up Provider Services. In the meantime, the Legislature could consider means to address the electric current gap in statewide back‑up provider services. For example, the Legislature could extend the expenditure authorization of any unspent funds originally provided for the temporary emergency dorsum‑upwardly provider organisation to June 30, 2022. (Recently, the administration extended the expenditure authority for existing essential protective gear funds from December 31, 2021 to June 30, 2022 via an all‑county letter. A similar approach could possibly be used to extend the expenditure authority of any unspent dorsum‑up provider service funds.) Alternatively, the Legislature could allow the $5 million General Fund allocated in the 2021‑22 budget to be used for emergency dorsum‑up provider services until a permanent organization is established or adopt the administration'south permanent back‑upward provider system proposal early (to the extent that the proposed language reflects Legislative goals).
Proposed Full‑Scope Medi‑Cal Expansion to
Remaining Undocumented Adults
LAO Bottom Line: Proposed Total‑Scope Medi‑Cal Expansion to Remaining Undocumented Adults Would Increase IHSS Caseload. Historically, income‑eligible undocumented immigrants only qualified for "restricted‑scope" Medi‑Cal coverage, which covers their emergency‑ and pregnancy‑related service costs. In general, beneficiaries of restricted telescopic Medi‑Cal are non eligible for IHSS. The country has expanded comprehensive, or "full‑scope," Medi‑Cal coverage, including IHSS eligibility, to income‑eligible undocumented children (effective May 2016), adults aged 19 through 25 (effective January 1, 2020), and older adults aged fifty and over (effective no sooner than May 2022).
The Governor's budget proposes to farther extend total‑telescopic Medi‑Cal coverage and IHSS eligibility to income‑eligible undocumented immigrants anile 26 to 49 no sooner than January 2024. Equally a event of this proposal, all undocumented immigrants, regardless of age, will be eligible for full‑scope Medi‑Cal and IHSS. While no funding is provided within the upkeep window (2021‑22 and 2022‑23) due to the proposed schedule of implementation, the administration estimates that this policy alter will increase IHSS costs over time, reaching ongoing costs of roughly $400 million General Fund in 2026‑27. (Upcoming publications, The 2022‑23 Budget: Analysis of the Medi‑Cal Budget and The 2022‑23 Upkeep: Analysis of Health Care Access and Affordability Proposals, will provide additional details on the full‑scope Medi‑Cal expansion to remaining undocumented adults.)
Implementation of Phasing in the Medi‑Cal Nugget Limit Repeal
LAO Bottom Line: Phasing in Medi‑Cal Asset Limit Repeal Will Increase IHSS Caseload. Currently, seniors and persons with disabilities must have assets at or below $2,000 (or $three,000 for couples) to be eligible for Medi‑Cal. The 2021‑22 budget included legislation to raises the Medi‑Cal nugget limit from $2,000 to $130,000 for individuals and from $3,000 to $195,000 for couples no sooner than July 2022. Moreover, the nugget limit would be eliminated altogether no sooner than Jan 2024 if the necessary federal approvals are obtained. The Governor's budget assumes that the asset limit volition be raised on July one, 2022, resulting in more seniors and persons with disabilities becoming eligible for Medi‑Cal services, including IHSS. The administration estimates that most 6,000 seniors and persons with disabilities will get eligible for IHSS as a result of this policy change, increasing Full general Fund costs by $67 1000000 in 2022‑23.
IHSS‑Related HCBS Spending Plan Items
LAO Lesser Line: DSS Working Towards Implementation of IHSS‑Related HCBS Spending Plan Items. As previously mentioned, the ARP Human activity temporarily increases the federal Medicaid friction match for HCBS services, including IHSS. The land expects to receive, in total, $iii billion in boosted federal Medicaid funds (including the estimated $one billion in additional federal Medicaid funds for the IHSS program). Equally a status of receiving these funds, the state is required to spend an equal amount of funding on new HCBS enhancements and expansions. The federal regime conditionally approved the various HCBS enhancements and expansions included in the state's HCBS spending plan. The land's HCBS spending plan includes ii IHSS‑related enhancements: (1) provide a one‑time $500 incentive payment to IHSS providers who worked at to the lowest degree two months between March 2020 and March 2021 and (2) create specialized training opportunities for IHSS providers. We understand that the one‑time $500 payments to IHSS providers tentatively are scheduled to occur in early on 2022. Additionally, DSS is currently seeking stakeholder input on the structure of the IHSS provider preparation opportunities, which is prepare to start no afterward than September ane, 2022 (and remain operative until March 1, 2024).

How Much Does In Home Supportive Services Pay,
Source: https://lao.ca.gov/Publications/Report/4512
Posted by: lomeliyousintor.blogspot.com
0 Response to "How Much Does In Home Supportive Services Pay"
Post a Comment